
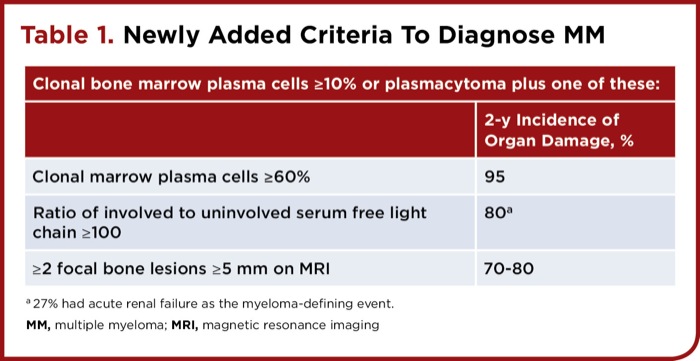
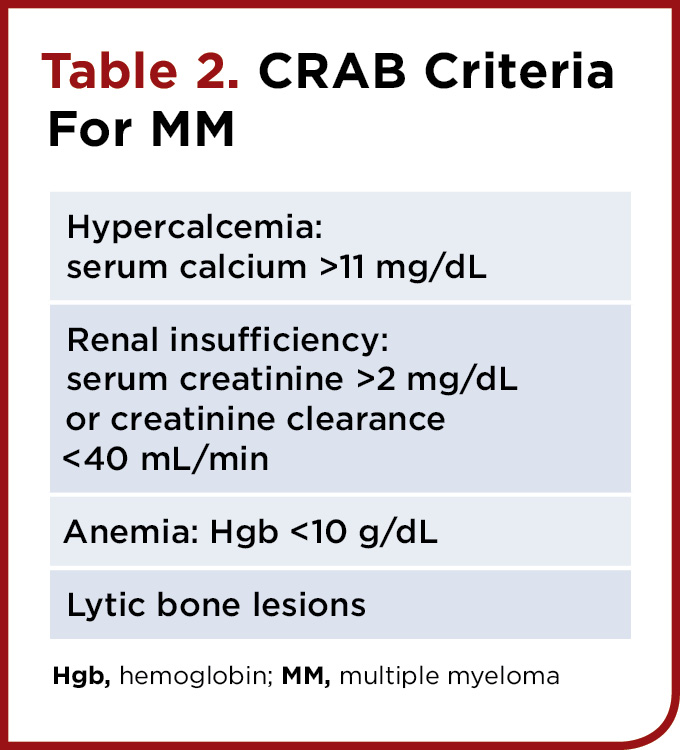
BY STEVEN VOGL, MD, Medical Oncologist, for Clinical Oncology In a thoughtful and precise paper, the International Myeloma Working Group (IMWG) last fall expanded the definition of multiple myeloma (MM) to include 3 groups of asymptomatic individuals as patients with the disease, because of data that each group is highly likely to develop organ or bone damage within 2 years (see Table 1). To my knowledge, there are no prospective trials indicating that immediate treatment of individuals meeting one of these 3 criteria who are asymptomatic and who do not meet the strict “CRAB” criteria for diagnosis of MM (Table 2) makes them live longer or better compared with waiting and watching carefully for an early sign that something is getting significantly worse. Treating these individuals, largely identified because routine blood tests showed a high globulin level, is not very different from giving multiagent chemotherapy to women with resected breast cancer with multiple involved axillary nodes. For the latter situation, we required multiple positive large clinical trials before adjuvant chemotherapy became standard practice. I recall bitter arguments among conscientious physicians in 1974 about adjuvant breast cancer chemotherapy. Many worried that women who would never relapse would be exposed to the ravages of multiagent chemotherapy.
|
||||||||||||||
Similarly, I initially worried that these new disease definitions might lead to frequent overtreatment, especially when decisions to treat the patient as overt MM are left to busy physicians who mechanically apply guidelines. On reflection, these considerations are outweighed by the benefits to thoughtful and conscientious physicians and their patients of expanding the disease definitions to include these ominous situations. Before the expanded definition, it was possible that payment for effective treatment of these patients would have been denied even when both patient and physician thought the patient would be best served by treatment. Payors May Insist Only Overt MM Deserves Expensive Drugs Although those of us who treat MM are delighted that we can do much better than give minimally effective (but cheap) melphalan and prednisone as initial treatment, the newer more effective treatments come with annual price tags that start at more than $100,000, putting them out of reach of patients without excellent insurance. If the definition of MM that needs treatment did not include these high-risk scenarios of what before was termed smoldering MM (SMM), then insurance companies may quickly discover that they can divert funds toward profits, rather than paying for bortezomib (Velcade, Takeda/Millennium) and lenalidomide (Revlimid, Celgene) for these patients. Drug companies are bringing ever more effective drugs to market. Alas, none are competing on price. Insurance companies, ever looking to the bottom line, are aware that if they deny treatment and the patient’s life is shortened, their expenditures may be lower as a result. Opponents of the revisions point out that so far no prescription plan has denied treatment for MM, whether it is smoldering or not, based on a failure to strictly meet the “CRAB” criteria. Additionally, SMM and overt MM share a billing code, as well as essentially identical bone marrow biopsy reports. As annual costs for each of several drugs leap over the $100,000 barrier, however, the incentive for insurance plans to scrutinize precise diagnoses increases exponentially.
|
Critics of the expanded definitions also point out that they are static, and that they ignore the clinician’s ability to carefully follow not only immunoglobulin levels and light-chain levels, but also hemoglobin as it falls from 12 toward 10, creatinine as it rises toward 2, and calcium as it rises between 10 and 10.9 mg/dL. These ominous trends would trigger many of us to treat a patient short of the CRAB criteria. The absence of such trends with near-normal and stable levels of hemoglobin, calcium, and creatinine might identify the 20% of individuals with light-chain ratios greater than 100 and the 30% of patients with 2 or more bone lesions at least 5 mm in diameter on magnetic resonance imaging (MRI) who will be progression-free 2 years later. Little is likely to be lost by watchful waiting in such patients, the critics argue, provided that observation is frequent and keen. It would be very useful to know the initial clinical characteristics of those who did not worsen enough to satisfy CRAB criteria 2 years into their observation periods, so we could especially consider a period of observation without intervention for patients like them. These critics fear that some individuals (admittedly a minority) will become MM patients on lifelong therapy by application of rigid criteria based on data that show that a majority are likely to progress within 1 to 2 years. My reply to the critics is that smart doctors will watch their patients carefully before committing them to chemotherapy. I hope that the members of the IMWG, as they speak at meetings and educational forums, will emphasize that the new diagnostic expansions are not engraved in stone, and that the presence of two 6-mm lesions on bone MRI does not mean that every such patient needs immediate systemic antimyeloma therapy. Indeed, in the Lancet Oncology paper, the IMWG favors repeat MRI in 3 to 6 months in questionable situations. What is not stated, but is assumed, is close follow-up of hemoglobin, creatinine, and calcium. How To Treat Asymptomatic Patients? There is little doubt that the myeloma clone can be effectively suppressed by modern chemotherapy when “CRAB” criteria are not met. In a Spanish trial of initial lenalidomide plus dexamethasone in unconventionally defined “high-risk” SMM, the overall response rate was 90%, including many remissions in which the paraprotein was no longer identifiable. For these individuals without symptoms or significant abnormalities in blood counts, kidney function, bones, and calcium level, one would like a treatment that is tolerable, easy to give outside of the hospital, unlikely to lead to severe symptoms or hospitalizations, and without long-term toxicities. I would favor low-dose dexamethasone (40 mg/wk) plus weekly bortezomib subcutaneously plus lenalidomide. Other tolerable regimens using just 2 drugs or incorporating newer agents, such as carfilzomib (Kyprolis, Onyx) and pomalidomide (Pomalyst, Celgene), also come to mind. These choices should be compared specifically in these lower burden myeloma patients. Having made MM better in the asymptomatic patient with no bone pain, we have no data on how long to treat the patient, whether to give bisphosphonates that reportedly prolong survival in overt MM, whether to consolidate at some point with high-dose melphalan rescued by autologous stem cells, when to collect these stem cells (early in treatment or after relapse just before high-dose melphalan), whether to administer expensive and somewhat toxic maintenance therapy with lenalidomide and/or bortezomib, and how long to give such maintenance therapy. Because these patients begin therapy with a largely lower disease burden and with disease that in many cases is less virulent (perhaps genetically or epigenetically), one cannot reasonably assume that data derived from treatment of overt MM will apply. These patients may have deeper or longer remissions and more drug-sensitive relapses than patients with overt MM at initiation of treatment, and so may derive less benefit from prolonged and toxic therapies. How Reproducible Are MRI Interpretations? Are Experts Available Everywhere? The IMWG has just published its comprehensive analysis of the MRI literature on which the MRI recommendation was based.4 The paper convinces the reader that in expert hands, multiple MRI lesions greater than 5 mm are a sign of imminent progression of disease in the majority of SMM patients. Nowhere in the paper is there a citation showing that MRI interpretations are reproducible from one radiologist to another, especially in the presence of hemangiomas, Schmorl’s nodes, or benign compression fractures. Breast pathologists routinely err about 15% of the time when interpreting estrogen receptors using immunohistochemistry—I would be surprised if even expert MRI radiologists had a concordance of greater than 85% in interpreting small areas of marrow heterogeneity. In the United States, it often is general radiologists with limited MRI experience who interpret MRI exams. Their concordance with a panel of experts would be expected to be less than 85%. The IMWG should assemble a panel of MRI images—positives, negatives, and some likely false-positives culled from among people with SMM—and circulate them to a panel to check concordance. If a high level of concordance can be established, members of the panel should make themselves available for reasonable fees to review MRI images from equivocal cases elsewhere or where MRI experts are not available. The IMWG stated that when doubt exists as to the interpretation of the MRI, when there is diffuse infiltration of uncertain significance, or when there is just one focal lesion, the study should be repeated in 3 to 6 months. Patients whose lesions do not worsen seem to do relatively well, they report. Repeat MRI is expensive but a bargain compared with immediate commitment to lifelong expensive therapy. The MRI study recommended by the IMWG is imaging of the total body, something not widely available in the United States. Whole-spine and pelvis MRI (which detects about 90% of the lesions found in the total-body study) is more widely available at the moment, and is likely the test that will be widely applied. Can Relatively Favorable Groups Be Defined Within The New MM Population? MM is heterogeneous in prognosis by cytogenetics, levels of normal immunoglobulins, levels of circulating plasma cells, percentage of abnormal plasma cells in marrow by multicolor flow cytometry, plasma cell proliferative rate, rate of paraprotein increase, and presumably other tests yet to be devised or applied to MM. Some of these tests may allow the identification of people with 2 or more marrow lesions on MRI who will progress slowly or not at all. These groups should be sought and the relevance of these prognostic factors tested prospectively. Will Some Interpret the New Definition as Demanding Immediate Treatment? Guidelines committees at the American Society of Hematology, the National Comprehensive Cancer Network, and elsewhere should support thoughtful, cautious clinicians who closely follow asymptomatic and stable patients without treatment, whether they meet the old CRAB criteria or the new expanded criteria. In my career, I have cared for 2 patients with overt MM, each with multiple lytic bone lesions and a big protein spike, who have been stable for decades off treatment—for reasons I cannot explain. Even though MM is a terrible disease for most people unless it is controlled long-term by effective therapy, we should continue to seek to identify those who do not need that therapy—close observation likely will be part of that process. IMWG Accepts Plain English Definition of ‘Symptomatic’ The Lancet Oncology paper finally makes clear that the serious disease that myeloma doctors treat is called MM. In the past, regardless of whether the patient was bothered by any symptoms or not, it was referred to as symptomatic MM, even if the patient had no complaints at all. For those of us who are not doctors specializing only in MM, the use of plain English removes a source of recurring confusion. In Philadelphia, they like to call myeloma needing treatment “active MM.” In this editorial, I have used the term “overt MM.” Approach to ‘At-Risk’ Asymptomatic Plasma Cell Dyscrasia When dealing with a patient who feels well, the smart, concerned clinician will always pause and be certain of parameters before committing the patient to lifelong therapy with a series of progressively more unpleasant therapies. Single laboratory findings should be confirmed, a disease trajectory should be established, and radiographic findings checked carefully by experienced interpreters before clinicians leap into therapy. On the other hand, a previously healthy patient who appears with 20% monoclonal plasma cells in the marrow, a creatinine of 1.9, a hemoglobin of 10.5, a calcium of 10.7, and 5 clear-cut bone lesions on MRI that clearly are not hemangiomas or Schmorl’s nodules can pretty safely be assumed to have a serious illness and be treated for overt MM, even though the patient denies symptoms and has no lytic lesions on bone films, especially if any of the abnormal lab findings are getting worse. For more information, click here.
about the author
Lizzy Smith
Lizzy Smith was diagnosed with myeloma in 2012 at age 44. Within days, she left her job, ended her marriage, moved, and entered treatment. "To the extent I'm able, I want to prove that despite life's biggest challenges, it is possible to survive and come out stronger than ever," she says.
More on Treatment Advances





Trending Articles








Get the latest thought leadership on Multiple Myeloma delivered straight to your inbox.
Subscribe to the weekly "HealthTree Community for Multiple Myeloma Newsletter" for Multiple Myeloma news, life with Multiple Myeloma stories, Multiple Myeloma clinical trials, Multiple Myeloma 101 articles and events with Multiple Myeloma experts.
Thanks to our HealthTree Community for Multiple Myeloma Sponsors:




Follow Us
Education
News Multiple Myeloma 101 My Journal University Expert Webinars Find a Specialist HealthTree PodcastCommunity
Connect Chapters Coach HealthTree Moves All Events Black Myeloma Health Resources in SpanishCure Hub
Cure Hub Side Effect Solutions Track Your Disease Connect Medical Records Treatment Options Twin Machine Clinical Trial Finder

HealthTree Foundation is a qualified 501(c)(3) tax-exempt organization.
Copyright © 2024 HealthTree Foundation. All rights reserved.
Tax ID 45-5354811